The United Nations health agency is calling for wider use of near point-of-care tests and tongue-swab sampling, arguing that faster, simpler tuberculosis diagnosis could help reach more patients and close one of the deadliest gaps in global infectious disease control.
GENEVA — The World Health Organization on March 24, 2026 called on countries to accelerate the rollout of new tuberculosis diagnostic tools, including tests that can be used near the point of care and easier sample collection through tongue swabs, in a push to detect cases earlier and reach more people who are still being missed by health systems.
The appeal, made on World TB Day, reflects an urgent reality: tuberculosis remains one of the world’s deadliest infectious diseases, despite being both preventable and curable. WHO says the disease caused 1.23 million deaths in 2024, including 150,000 among people living with HIV, and that 10.7 million people fell ill with TB that year. The agency describes TB as the leading cause of death from a single infectious agent worldwide and among the top 10 causes of death overall.
Those figures help explain why changes in diagnosis matter so much. For global health officials, one of the biggest barriers to controlling tuberculosis is not only treatment access, but the failure to identify patients quickly enough. Delayed diagnosis means delayed treatment, greater risk of transmission and worse outcomes for patients, especially in settings where health systems are stretched and laboratory infrastructure is limited.
WHO’s latest recommendations are aimed squarely at that problem. The agency is urging countries to use new near point-of-care molecular tests that can bring faster diagnosis closer to where patients first seek care, rather than relying only on centralized laboratories that can be slow, hard to access or unavailable in rural and low-resource areas.
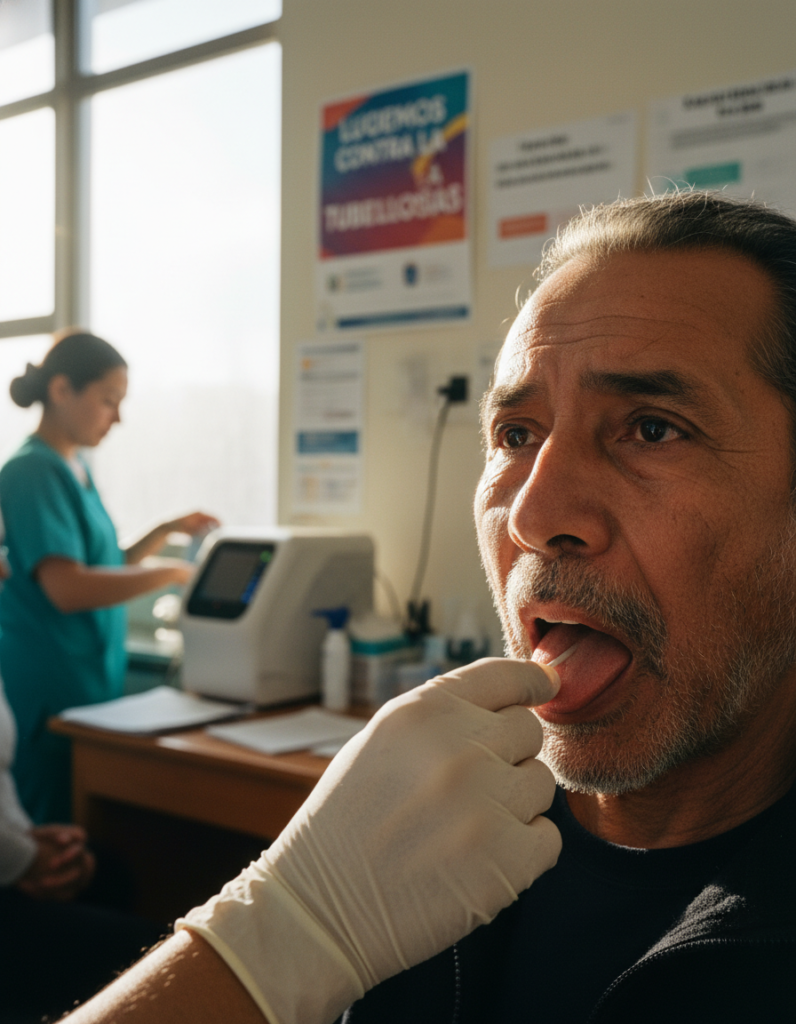
The organization is also recommending the use of tongue-swab samples in specific circumstances, especially for adults and adolescents with signs and symptoms of pulmonary TB who cannot produce sputum. For many patients, sputum collection has long been a practical obstacle in diagnosis. Producing a good-quality sample can be difficult, particularly for some older patients, children, people who are very ill, and others who cannot cough up sputum on demand. The ability to use a simple swab from the tongue could therefore widen access to testing for people who might otherwise go undiagnosed.
WHO says the updated recommendations also include sputum pooling, a cost-saving strategy intended to increase testing efficiency. Together, the changes are designed to make diagnosis faster, more accessible and more adaptable to real-world clinical settings where staff, time and resources are often constrained.
The significance of the announcement lies not only in the technologies themselves, but in what they represent for global TB control. Tuberculosis has long been a disease of inequity. It thrives in crowded conditions, disproportionately affects low- and middle-income countries, and often strikes people facing poverty, undernutrition, weak health access or other vulnerabilities. In many places, the people most at risk are also the least likely to receive timely, high-quality testing.
That is why moving diagnostic tools closer to the patient has become a major goal of TB policy. Near point-of-care testing can reduce the number of visits required, shorten turnaround times and lower the chances that patients are lost somewhere between screening, sample collection, lab processing and treatment initiation. In theory, that means more people can be diagnosed at an earlier stage and started on life-saving therapy before they become sicker or infect others.
WHO linked the recommendations to the broader goals of its End TB Strategy and the political commitments made at the United Nations High-Level Meeting on tuberculosis. Countries have already committed to expanding early diagnosis and universal access to rapid molecular testing. Yet the agency says major diagnostic gaps persist, leaving many cases undetected or diagnosed too late.
For clinicians and public health officials, the tongue-swab recommendation may be one of the most closely watched elements of the new guidance. It points to a future in which TB testing can become less invasive and easier to scale. While sputum remains central to many forms of TB diagnosis, the new recommendation acknowledges a basic clinical challenge: some people simply cannot provide it when needed. By allowing tongue swabs to be used with low-complexity automated molecular tests in people who cannot produce sputum, WHO is widening the diagnostic doorway.
That could have practical implications far beyond convenience. In crowded clinics or under-resourced health posts, simpler sample collection may help reach patients who would otherwise be sent away, delayed or never fully tested. It may also help bring testing into settings where conventional sputum-based workflows are difficult to maintain.
The new guidance comes at a time when TB control is facing both opportunity and strain. WHO’s Global Tuberculosis Report 2025 showed that although some progress has continued, the epidemic remains far from over. The disease is still a major killer of people living with HIV and an important contributor to deaths associated with antimicrobial resistance. At the same time, WHO has warned that funding pressures and broader health system disruptions threaten to slow momentum in many countries.
That makes implementation the next major question. WHO’s announcement is a policy signal, but turning recommendations into real-world access will depend on national procurement, training, quality assurance, financing and the practical readiness of health systems. New tools are only as effective as the networks that deliver them. Machines must be available, staff must know how to use them, supplies must be consistent, and patients must be able to move from diagnosis to treatment without delay.
The challenge is particularly acute in high-burden countries, where the need is greatest and the margins for failure are narrow. If countries can integrate these tools successfully into routine care, they could close part of the long-standing gap between innovation and access that has defined much of the TB response.
There is also a communications challenge. Tuberculosis rarely captures the same sustained public attention as sudden outbreaks, even though it kills on a scale that makes it one of the most consequential infectious diseases on the planet. Because TB is both ancient and treatable, it can fade from view politically. WHO’s World TB Day message appears intended to counter that complacency by framing diagnosis as an urgent frontline issue, not a technical afterthought.
The language of the agency’s March 24 appeal was notably practical. Rather than presenting the recommendations as a futuristic leap, WHO positioned them as tools that can help countries reach more people now. The emphasis was on acceleration, access and service delivery: getting diagnosis closer to patients, simplifying sample collection and using innovations that fit real health systems rather than idealized ones.
That may be why the announcement matters beyond specialist circles. In global health, the most important breakthroughs are not always brand-new medicines or headline-grabbing scientific discoveries. Sometimes they are improvements in the way existing care is delivered — faster, closer, more simply and to more people. In tuberculosis, where late diagnosis remains one of the central obstacles to control, such changes can alter the course of both individual illness and community transmission.
WHO’s message on World TB Day was ultimately a reminder that ending TB is not only about having treatment. It is about finding people in time.
If near point-of-care testing, tongue-swab sampling and more efficient testing strategies can help countries do that at scale, they may become one of the most consequential shifts in TB care in years. For a disease that still kills more than a million people annually, the ability to diagnose earlier is not a marginal improvement. It is a central test of whether global promises to end tuberculosis can be turned into reality.
